Delirium or sudden confusion
Delirium is sudden, acute or intense confusion and it can affect anyone when they are very unwell, but is much more likely in a person with dementia. It is treatable and reversible.
It can be frightening if the person you are caring for shows symptoms of delirium, which may cause them to act very differently. It’s important to go and see your GP as soon as possible as it can be treated. Lorraine Haining, Specialist Dementia Nurse, Dementia Carers Count
Delirium or sudden confusion
Delirium is sudden, acute or intense confusion and it can affect anyone when they are very unwell, but is much more likely in a person with dementia.
One of the challenges with identifying delirium is that it comes with very varied behaviour, but if you suspect delirium in any way, it is important you act on it.
It occurs suddenly, within hours or days, and can be very frightening for both the person affected and those caring for them.
Why it’s important to treat delirium
Delirium needs to be addressed and treated as early as possible as it can have serious negative consequences. One episode can increase the risk of further episodes, especially if it goes untreated.
If you are an older person and have other pre-existing health conditions as well as dementia, your mortality risk increases if you develop delirium.
Acting quickly can make a difference.
Symptoms of delirium
There are different types of delirium. These are sometimes called hyperactive delirium, hypoactive delirium or mixed delirium.
Hyperactive delirium
Hyperactive delirium is the most obvious kind with very marked, sudden and major changes in how the person acts.
The person may be agitated or abnormally active. This may include:
- constant monitoring of potential threats around them (hypervigilance)
- restlessness
- rambling speech
- being startled by loud noises and over-reacting in response to them
- hallucinations
- wandering
- being distracted
- being irritable or showing low tolerance of frustration
Due to confusion and anxiety, they may become defensive and react with verbal or physical threats against people who try to help them.
Hypoactive delirium
Hypoactive delirium is much less obvious. It is marked by a decrease in behaviour or physical activity.
The person may seem sleepy and inactive, speaking more slowly and being less aware of their surroundings.
It can often be mistaken for depression or a deterioration in a person who already has dementia, rather than a separate issue that needs treating.
A person may display a mixture of hyperactive and hypoactive delirium, switching between the two.
Why does it happen?
The most common causes of delirium are:
- Being aged over 65
- A urine or chest infection
- Having a high body temperature
- Side effects of drugs, like pain killers and steroids
- Chemical problems in the body, such as dehydration or low salt levels
- Liver or kidney problems
- Suddenly stopping drugs or alcohol
- Major surgery -especially hip and vascular surgery
- Epilepsy
- Brain injury or infection
- Terminal illness
- Constipation
- Use of an indwelling catheter
- Being in an unfamiliar place.
- Pain
- Lack of mobility (often due to a fall)
There is often more than one cause – and sometimes the cause is not found.
What to do for a person with delirium
Being aware of the symptoms of delirium, picking up on them and going straight to your GP when you notice them is the most important thing you can do. Your GP can then look into what might be causing the delirium and make sure it is treated. Lorraine Haining, Dementia Specialist Nurse
The most important first step for a person with delirium is to recognise they are experiencing it.
Being aware of risk factors and making sure they are under control and treated is also important.
For example, if the person has a urinary tract infection or a high temperature, get it treated as soon as possible to help stop delirium from happening in the first place.
Be aware of early warning signs
Over time you may become aware of the early warning signs of delirium in the person you are caring for, especially as you know their personality better than other people. It is good in this case to write these early warning signs down. You can pass the information on to anyone else who cares for them, in hospital or at home.
If the person is prone to bouts of delirium, or one of their risk factors has come into play, make sure their environment is as calm as possible.
How can I help someone with delirium?
Looking after yourself
A person experiencing delirium can become quite nasty or aggressive to the people around them or caring for them due to the symptoms of hallucination and delusions (vivid visions or dreams).
They will feel threatened or fearful and might accuse you of stealing from them or trying to hurt them in some way.
Hallucinations may keep them in a constant state of fear. A person with delirium may think much more time has passed than is true in the ‘real’ world. These beliefs will seem real to the person and they will not be able to tell they are not real.
These symptoms are beyond their control, but if it is happening frequently, it can be very upsetting for you as a carer.
Coping with hallucinations and delusions
The best thing you can do in this situation, apart from getting the cause of the delirium treated, is to try and make sure you are getting some time out from caring for the person to give yourself time to recover emotionally.
Try asking family or friends to support you to give you some time away from the situation.
If this isn’t possible, even stepping outside of the room and taking a deep breath can help. Talking to someone about what you are dealing with can also make things feel more manageable.
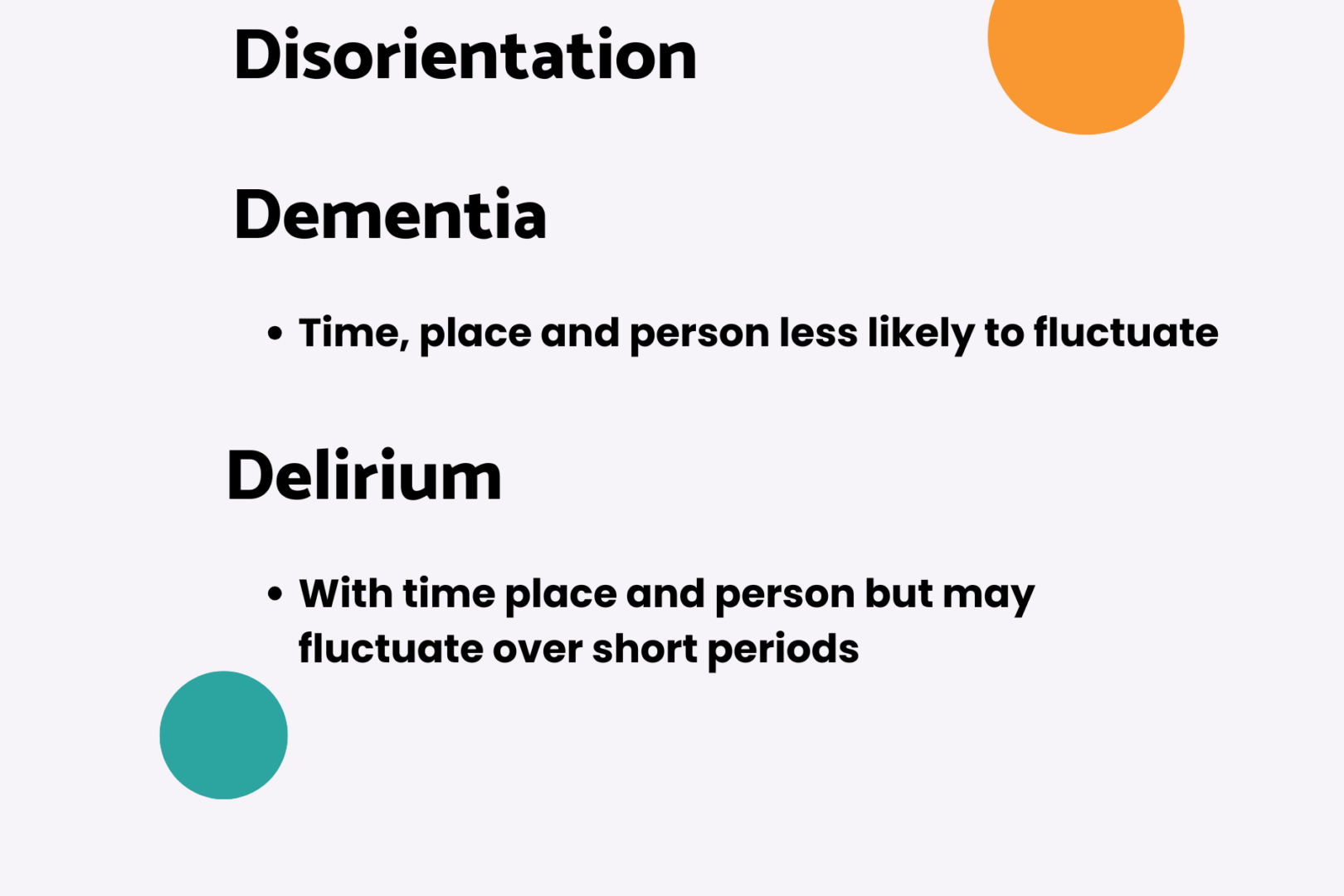
The difference between delirium and dementia
The difference between delirium and dementia isn’t always clear, even for professionals, because it’s possible that delirium happens on top of dementia, but there are some differences.
While dementia is an ongoing condition, with gradual changes over time, delirium starts suddenly and is reversible. Lorraine Haining, Dementia Specialist Nurse
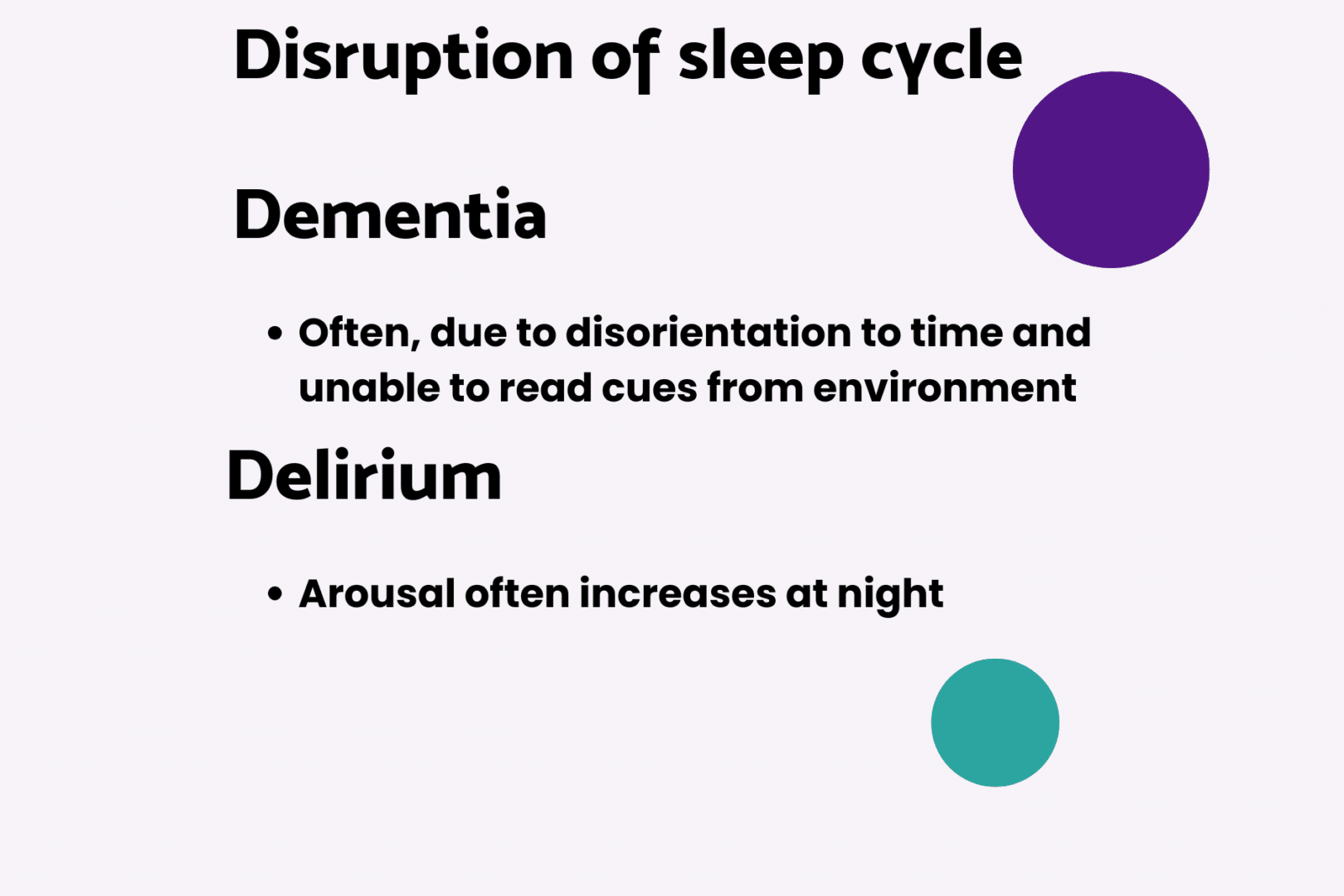
Overactive or hard to wake
A person with delirium can fluctuate between being overactive and hard to wake. A person with dementia keeps a more steady state of activity.
Hallucinations
Delirium frequently causes hallucinations or illusions. These are rare in someone with dementia, unless they have Parkinson’s or Lewy Body dementia.
Speech
Speech may be slow and incoherent in a person with delirium, while a person with dementia tends to repeat themselves and have difficulty finding words.
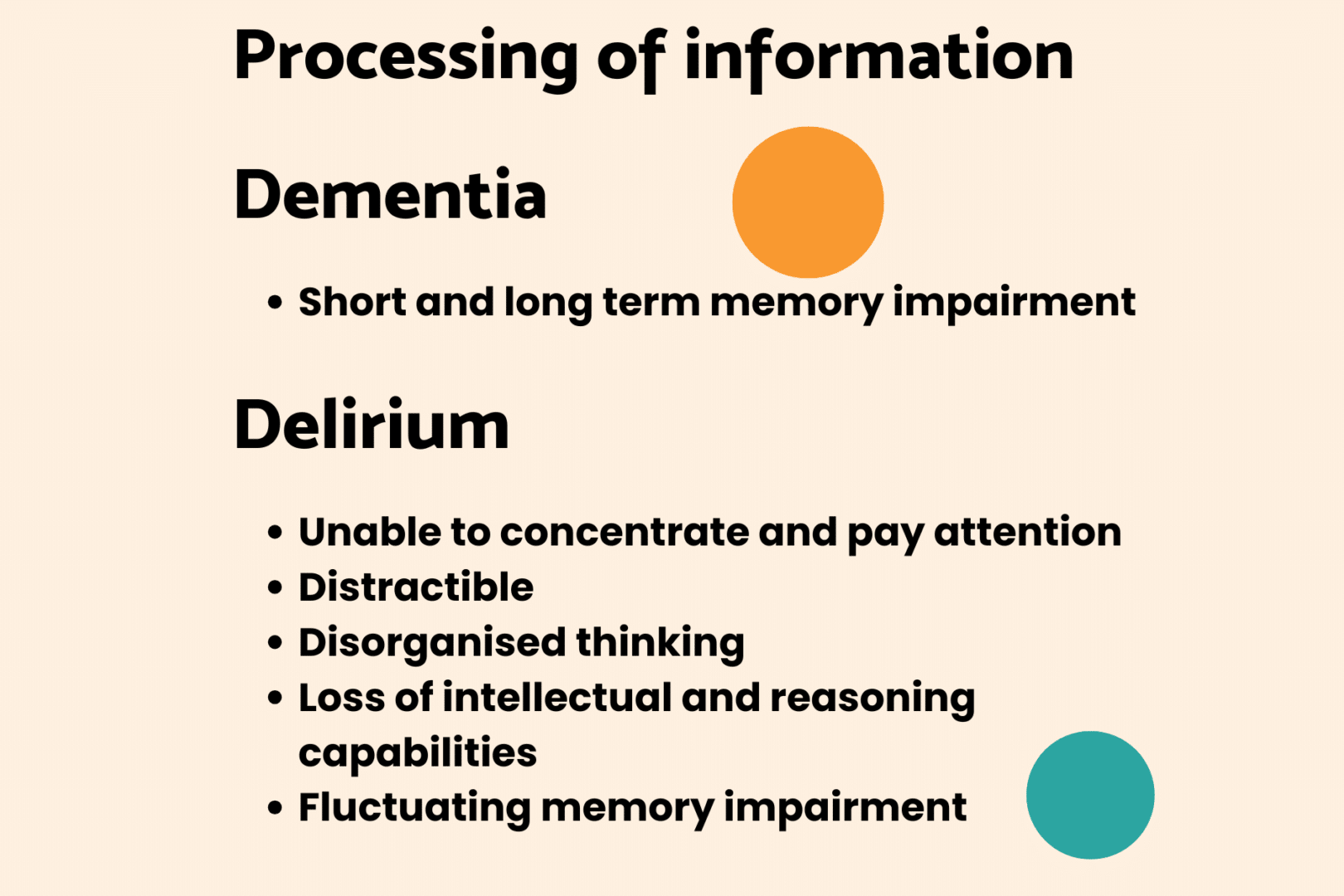
Concentration
A person with delirium may find it difficult to concentrate and pay attention. They may temporarily lose their ability to reason. A person with dementia will suffer short and long term loss of memory.
Delirium or sudden confusion






Getting a diagnosis
If you suspect someone has delirium, then an assessment and appropriate tests should be carried out as soon as possible. There can be multiple triggers/causes which can make diagnosis and treatment complex. It may take time to diagnose, so the earlier you seek help, the better the outcome for the person.
The person with delirium may be too confused to describe what has happened to them, so it’s important that the doctor can talk to someone who knows the person well.
Delirium diagnosed in hospital
About 1 in 10 hospital patients have a period of delirium. If delirium is diagnosed in hospital, it’s very important that the person’s GP is informed of the diagnosis. The GP may need to follow up and monitor the situation in the community.
How does the person feel afterwards?
They may not remember what has happened, particularly if they had memory problems beforehand. However, they may be left with unpleasant and frightening memories – and even worry that they are going mad.
It can be helpful to sit down with someone who can explain what happened. This might be a family member, a carer or a doctor. They can go through a diary of what happened each day.
Most people feel relieved when they understand what happened and why.
Recovery time
Once the cause of delirium is identified and treated, it usually goes away. The recovery time is different for each person. They can get better within hours or days depending on how quickly the delirium is recognised and treated.
However, in about one in five people, it can last for weeks or months. People with dementia can take a particularly long time to get over delirium.
Will it happen again?
After a first episode of delirium, it’s very helpful to have a prevention plan in place. The person is more likely to have delirium again if they become medically unwell. A prevention plan will help you to recognise any early warning signs, seek treatment quickly and prevent escalation.
Talk to hospital staff, your local GP or community mental health team who may already have specific care plans in place.
The effect of delirium on you as a carer
As a carer, delirium can have a big impact on you and your emotional wellbeing.
Knowledge really is power in these circumstances. So make sure you get the right information, keep up to date, ask questions and make your needs known by asking for a carer’s assessment.
Don’t be afraid to voice your concerns for the person you care for as they may not be able to, but also for yourself and your own ability to cope. Lorraine Haining, Dementia Specialist Nurse
Read Next
Stress and distress
As a person’s dementia increases, there are many factors that might increase the likelihood of them experiencing stress and showing distress. Understanding and tackling the causes of stress can help carers cope.

Ways to support communication
Dementia can affect a person’s ability to communicate but there are ways to support communication to make connecting easier.

How dementia affects memory
Dementia often affects memory. There are things you can do to support the person you care for if they are experiencing memory problems.
